Drug name
Last update: Jul 2026Cabotegravir (CAB)
Developer(s)
Drug information
Cabotegravir
Apretude, Vocabria
Small molecule
integrase strand transfer inhibitor; INSTI)
Cabotegravir (CAB), also known as GSK1265744, is a HIV-1 integrase strand transfer inhibitor (INSTI). Long-acting versions of CAB (CAB-LA) are currently administered once monthly or every-2-months as a intramuscular (IM) injection containing an extended-release drug particle nanosuspension, with an optional ~30 day oral-lead in period. CAB-LA administered by IM injection requires approximately one week to achieve maximal plasma drug concentration. CAB is metabolised in the body by the enzyme UGT1A1; with the average half-life of IM CAB-LA ranging from 5.6 to 11.5 weeks.
An injectable formulation of cabotegravir is approved for use for HIV PrEP and as part of a regimen, for HIV treatment
Cabotegravir LA, both as suspension for intramuscular injection 600mg/3ml (200mg/ml) and as 30 mg tablet is included in WHO PQ: https://extranet.who.int/prequal/sites/default/files/document_files/EOI_23rd%20HIV_9July_2025_clean_PQ.pdf Cabotegravir for PrEP is included in WHO guidelines. CAB+RPV LA injectable for treatment, is also recommended by WHO to be used as an alternative switching option for adults and adolescents with undetectable HIV viral load on oral ART and without active hepatitis B infection : https://www.who.int/teams/global-hiv-hepatitis-and-stis-programmes/guidelines ViiV Healthcare and Medicines Patent Pool have signed a voluntary licensing agreement to enable access to long-acting injectable cabotegravir for HIV PrEP and HIV treatment
Therapeutic area(s)
- HIV
- Pre-Exposure Prophylaxis (PrEP)
- Treatment
Administration route
Oral, Intramuscular, Subcutaneous
Associated long-acting platforms
Aqueous drug particle suspension
Use of drug
- Administered by a nurse
- Administered by a specialty health worker
- Administered by a community health worker
- Self-administered
- To be determined
- Daily
- Monthly
- Every 2 months
- Other/Variable/Unknown : Other investigated formulations may provide additional dosing frequencies
- Every 4 months
For prevention, CAB-LA is well accepted across key populations: in HPTN 083 (MSM/transgender women) and HPTN 084 (African cisgender women, including adolescent girls), adherence to scheduled injections was high and most participants preferred injectable over oral PrEP, citing discretion and freedom from daily pill-taking, though injection-site pain and clinic dependence were recurring concerns. For treatment, ATLAS and FLAIR showed that CAB+RPV LA produced significantly greater gains in treatment satisfaction and acceptance than daily oral ART, with ≥97% preferring injections over previous tt.
Dosage
Not provided
Not provided
Not provided
Not provided
Not provided
Associated technologies
Dissolving microarray patchesTunable Biodegradable Ultra-Long-Acting Polymeric Solid Implant (PSI)
Ultra-Long-Acting Multi-Purpose In-situ Forming Implant (ISFI)
DelSiTech Silica Matrix Drug Delivery
Peptide-like hydrogels as a long-acting injectable drug delivery platform
LYNX
Nanocrystalline Prodrug Technology
Comment & Information
Developer(s)

ViiV Healthcare
ViiV Healthcare is a pharmaceutical company that specializes in the development of therapies for HIV infection. The company is headquartered in Brentford in the United Kingdom and was initially formed in November 2009 as a part of a joint venture between GlaxoSmithKline and Pfizer.
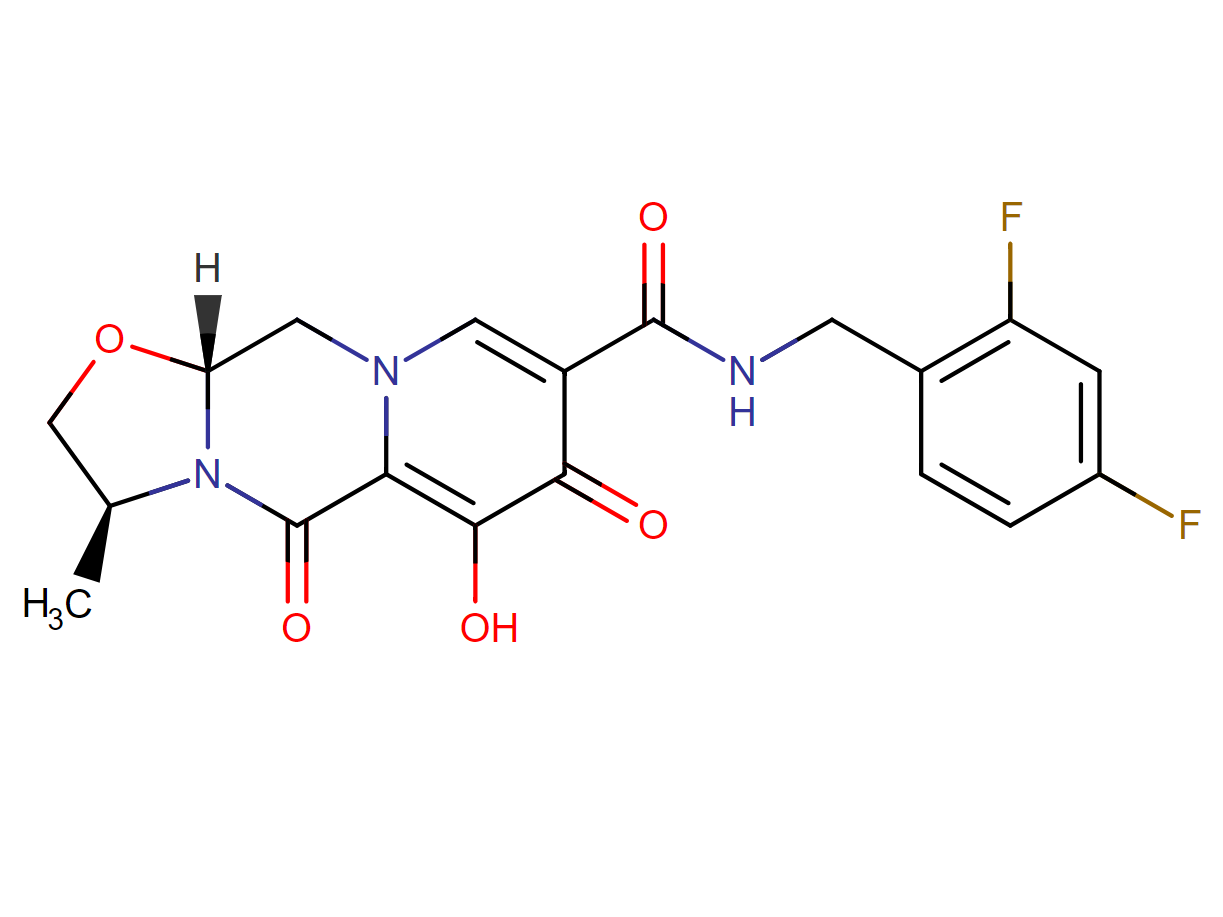
Drug structure
Scale-up and manufacturing prospects
Not provided
Not provided
Not provided
Not provided
Excipients
Mannitol (E421), polysorbate 20, macrogol 3350, water for injectable preparations ad solutionem pro 1 ml.
No novel excipient or existing excipient used
No residual solvent used
Delivery device(s)
No delivery device
Publications
Bowers GD. et al. : Disposition and metabolism of cabotegravir: a comparison of biotransformation and excretion between different species and routes of administration in humans. Xenobiotica. 2016
1. Cabotegravir [(3S,11aR)-N-[(2,4-difluorophenyl)methyl]-6-hydroxy-3-methyl-5,7-dioxo-2,3,5,7,11,11a-hexahydro[1,3]oxazolo[3,2-a]pyrido[1,2-d]pyrazine-8-carboxamide] is an HIV-1 integrase inhibitor under development as a tablet for both oral lead-in therapy and long-acting (LA) injectable for intramuscular dosing.
2. Metabolism, pharmacokinetics and excretion were investigated in healthy human subjects who received either a single oral dose (28.2 mg) of [14C]cabotegravir in a mass balance study, or LA formulations of unlabeled cabotegravir (200–800 mg), intramuscularly or subcutaneously, in a separate study. Metabolism, distribution and excretion of [14C]cabotegravir were also investigated in mice, rats and monkeys.
3. Recovery of radioactivity in humans represented a mean total of 85.3% of the dose, including 26.8% in the urine. The mean apparent terminal phase half-life was similar for both cabotegravir and radioactivity, 39 h compared to 41 h.
4. Following oral, intramuscular and subcutaneous administration, cabotegravir was the major component in plasma and the glucuronic acid conjugate (M1) represented the predominant component in urine. Cabotegravir was present in bile along with its major metabolite (M1).
5. The primary metabolite of [14C]cabotegravir in mouse, rat and monkey was the same as that in human. In vitro phenotyping experiments demonstrated that cabotegravir was metabolized by UDP-glucuronosyltransferase (UGT) 1A1 and UGT1A9.
Spreen W. et al, : Pharmacokinetics, safety, and monotherapy antiviral activity of GSK1265744, an HIV integrase strand transfer inhibitor. HIV Clin Trials. 2013 Sep-Oct;14(5):192-203. doi:
Background: GSK1265744 is an HIV integrase strand transfer inhibitor selected for clinical development.
Objective: This first-time-in-human and phase IIa investigation assessed GSK1265744 antiviral activity, pharmacokinetics, safety, and tolerability in healthy and HIV-1-infected subjects.
Methods: This double-blind, placebo-controlled study consisted of a dose escalation of single (part A) and multiple (part B) oral doses in 48 healthy subjects and an oral dose (part C) in 11 HIV-1-infected subjects. In part A, 2 cohorts of 9 subjects received either 5 and 25 mg or 10 and 50 mg. In part B, 3 cohorts of 10 subjects received 5, 10, or 25 mg once daily for 14 days. In part C and the phase IIa study, subjects received 5 or 30 mg once daily for 10 days.
Results: Dose-proportional increases in drug exposure were observed in healthy and HIV-1-infected subjects. In healthy subjects, pharmacokinetic variability was low following single or repeat dosing (coefficient of variation, 13%-34% and 15%-23%, respectively). Mean plasma half-life was 31.5 hours. GSK1265744 monotherapy significantly reduced plasma HIV-1 RNA from baseline to day 11 in HIV-1-infected subjects receiving 5 or 30 mg versus placebo (P < .001); mean decrease was 2.2 to 2.3 log10 copies/mL, respectively. Study drug was generally well tolerated with no clinically relevant trends in laboratory values, vital signs, or electrocardiograms.
Conclusions: GSK1265744 was well tolerated in healthy and HIV-1-infected subjects. Results demonstrate once-daily doses of 5 or 30 mg exceeded minimum target therapeutic concentrations and produced a significant reduction in plasma HIV-1 RNA viral load.
Trezza C. et al.. Formulation and pharmacology of long-acting cabotegravir. Curr Opin HIV AIDS. 2015 Jul;10(4):239-45. doi: https://doi.org/10.1097%2FCOH.0000000000000168. PMID: 26049948; PMCID: PMC5638427.
Purpose of review
Long-acting cabotegravir may provide a novel therapeutic option for both the treatment and prevention of HIV-1 infection that does not necessitate adherence to a daily regimen. The present review will highlight the unique formulation properties and pharmacologic attributes of long-acting cabotegravir nanosuspension.
Recent findings
Cabotegravir is a potent integrase strand transfer inhibitor that has been formulated as an oral tablet for daily administration and as a long-acting injectable nanosuspension. Long-acting cabotegravir is readily absorbed following intramuscular and subcutaneous administration and has an elimination half-life of approximately 40 days, allowing for administration on a monthly or less frequent schedule. Repeat-dose pharmacokinetic studies and population pharmacokinetic modeling indicate monthly and bi-monthly dosing achieves clinically relevant plasma concentrations considered effective for HIV maintenance therapy and that quarterly injections are appropriate for investigation as preexposure prophylaxis. Cabotegravir is primarily metabolized by uridine diphosphate glucuronosyltransferase 1A1 and is unlikely to be impacted by the cytochrome P450 metabolic pathway. In vitro and in vivo data suggest cabotegravir has a low propensity to cause, or be subject to, significant drug interactions.
Summary
The pharmacologic profile of long-acting cabotegravir supports its continued development for both treatment and prevention of HIV-1 infection.
Oka S, et al. Asian participants' experience in phase 3/3b studies of long-acting cabotegravir and rilpivirine: Efficacy, safety, pharmacokinetic, and virological outcomes through week 96. HIV Med. 2024;25(3):381‐390. doi:10.1111/hiv.13588
Overall, 41 Asian participants received CAB + RPV (Q8W, n = 17; Q4W, n = 24). At week 96, 83% (n = 34/41) of participants maintained HIV-1 RNA <50 copies/mL, none had HIV-1 RNA ≥50 copies/mL, and 17% (n = 7/41) had no virological data. No Asian participant met the CVF criterion. Drug-related adverse events occurred in 44% (n = 18/41) of participants; none were Grade ≥3. All injection site reactions were Grade 1 or 2; median duration was 2 days and most resolved within 7 days (90%, n = 390/435). CAB and RPV trough concentrations remained well above their respective protein-adjusted 90% inhibitory concentrations (CAB, 0.166 μg/mL; RPV, 12 ng/mL) through week 96.
Damschroder LJ. et al., Fostering implementation of health services research findings into practice: a consolidated framework for advancing implementation science. . Implement Sci. 2009;4:50. Published 2009 Aug 7. doi:10.1186/1748-5908-4-50
The CFIR provides a pragmatic structure for approaching complex, interacting, multi-level, and transient states of constructs in the real world by embracing, consolidating, and unifying key constructs from published implementation theories. It can be used to guide formative evaluations and build the implementation knowledge base across multiple studies and settings.
Proctor E, et al., Outcomes for implementation research: conceptual distinctions, measurement challenges, and research agenda. Adm Policy Ment Health. 2011;38(2):65-76. doi:10.1007/s10488-010-0319-7
An unresolved issue in the field of implementation research is how to conceptualize and evaluate successful implementation. This paper advances the concept of "implementation outcomes" distinct from service system and clinical treatment outcomes. This paper proposes a heuristic, working "taxonomy" of eight conceptually distinct implementation outcomes-acceptability, adoption, appropriateness, feasibility, fidelity, implementation cost, penetration, and sustainability-along with their nominal definitions. We propose a two-pronged agenda for research on implementation outcomes. Conceptualizing and measuring implementation outcomes will advance understanding of implementation processes, enhance efficiency in implementation research, and pave the way for studies of the comparative effectiveness of implementation strategies.
Orkin C., et al., Perspectives of People With HIV on Implementing Long-acting Cabotegravir Plus Rilpivirine in Clinics and Community Settings in the United Kingdom: Results From the Antisexist, Antiracist, Antiageist Implementing Long-acting Novel Antiretrovirals Study, Clinical Infectious Diseases, Volume 80, Issue 5, 15 May 2025, Pages 1103–1113,
Introduction
The equity-focused Implementing Long-Acting Novel Antiretrovirals study evaluated feasibility, acceptability, appropriateness of delivering on-label 2-monthly cabotegravir and rilpivirine (CAB + RPV) injections for human immunodeficiency virus (HIV)-1 therapy in clinics and community settings.
Methods
The study, which mandated inclusive recruitment, was conducted May–December 2022 at 6 UK sites. Injections were delivered in clinic (month [M] 1–6) and in clinic or community setting according to patient choice (M6–12). Surveys were completed at baseline, M4, and M12 using validated measures for feasibility (FIM), acceptability (AIM), and appropriateness (IAM). Primary endpoint: proportion of participants agreeing that the injection and community setting were feasible (FIM ≥4) at M12. Fourteen participants completed interviews at baseline and M12.
Results
Community settings offered by sites included: home visits (n = 3), HIV support organizations (n = 2), and community clinic (n = 1). Of 114 participants, 54% were female, 70% racially minoritized, and 40% aged ≥50 years. A total of 27/114 chose to receive injections in community settings. FIM/AIM/IAM scores at M12 were high for the injection (79.0–87.4%) and lower for the community setting (44.2–47.4%) overall. Subgroup analyses indicated differences in scores by gender and ethnicity. Among those who attended the community, FIM/AIM/IAM scores for the community setting at M12 were high (73.1–80.8%). Concerns about stigma, inconvenience, and losing access to trusted clinicians negatively influenced perceptions of receiving injections at community settings, amongst other factors.
Conclusions
CAB + RPV injections were considered highly feasible, acceptable, and appropriate; however, few chose community delivery. Those that chose community delivery found it highly acceptable and feasible. Further exploration of CAB + RPV delivery in alternative community sites not offered (eg, primary care, pharmacies) is warranted.
John M, Williams L, Nolan G, Bonnett M, Castley A, Nolan D. Real-world use of long-acting cabotegravir and rilpivirine: 12-month results of the inJectable Antiretroviral therapy feasiBility Study (JABS). HIV Med. 2024; 25(8): 935-945. doi:10.1111/hiv.13647
Objectives
The inJectable Antiretroviral feasiBility Study (JABS) aimed to evaluate the implementation of long-acting regimens in a ‘real world’ Australian setting, with inclusion of participants with complex medical needs, social vulnerability and/or historical non-adherence.
Methods
JABS was a 12-month, single-centre, single-arm, open-label phase IV study of long-acting cabotegravir 600 mg plus rilpivirine 900 mg administered intramuscularly every 2 months to adults with treated HIV-1 infection. The primary endpoint was the proportion of attendances and administration of injections within a 14-day dosing window over 12 months, out of the total prescribed doses. Secondary endpoints included proportions of missed appointments, use of oral bridging, discontinuations, virological failures, adverse events and participant-reported outcomes. A multidisciplinary adherence programme embedded in the clinical service known as REACH provided support to JABS participants.
Results
Of 60 participants enrolled by May 2022, 60% had one or more complexity or vulnerability factors identified, including absence of social supports (50%), mental health issues, alcohol or drug use (30%) and financial hardship or instability (13%), among others. Twenty-seven per cent of participants had historical non-adherence to antiretroviral therapy. Out of 395 prescribed doses, 97.2% of injections were administered within correct dosing windows at clinic visits. Two courses of short-term oral bridging were required. The rate of injection site reactions was 29%, the majority being grade 1–2. There were no virological failures, no serious adverse events and only one injection-related study discontinuation. High baseline treatment satisfaction and acceptability of injections increased by month 12. Those with vulnerability factors had similar adherence to injections as those without such factors. Ninety-eight per cent of the participants who completed 12 months on the study have maintained long-acting therapy, virological suppression and retention in care.
Conclusions
Long-acting cabotegravir plus rilpivirine was associated with very high adherence, maintenance of virological suppression, safety and treatment satisfaction in a diverse Australian clinic population, comparable to results of phase III randomized clinical trials. Individuals with vulnerability factors can achieve adherence to injections with individualized support. Long-acting therapies in this group can increase the subsequent engagement in clinical care.
Switch to long-acting cabotegravir and rilpivirine in virologically suppressed adults with HIV in Africa (CARES): week 48 results from a randomised, multicentre, open-label, non-inferiority trial. Kityo Cissy, Mugerwa Henry et al. The Lancet Infectious Diseases, Volume 24, Issue 10, 1083 - 1092
Background
Long-acting injectable cabotegravir and rilpivirine is licensed for individualised treatment of HIV-1 infection in resource-rich settings. Additional evidence is required to support use in African treatment programmes where demographic factors, viral subtypes, previous treatment, and delivery and monitoring approaches differ. The aim of this study was to determine whether switching to long-acting therapy with injections every 8 weeks is non-inferior to daily oral therapy in Africa.
Methods
CARES is a randomised, open-label, non-inferiority trial being conducted at eight sites in Uganda, Kenya, and South Africa. Participants with HIV viral load below 50 copies per mL on oral antiretroviral therapy and no history of virological failure were randomly assigned (1:1; web-based, permuted blocks) to receive cabotegravir (600 mg) and rilpivirine (900 mg) by intramuscular injection every 8 weeks, or to continue oral therapy. Viral load was monitored every 24 weeks. The primary outcome was week 48 viral load below 50 copies per mL, assessed with the Food and Drug Administration snapshot algorithm (non-inferiority margin 10 percentage points) in the intention-to-treat exposed population. This trial is registered with the Pan African Clinical Trials Registry (202104874490818) and is ongoing up to 96 weeks.
Findings
Between Sept 1, 2021, and Aug 31, 2022, we enrolled 512 participants (295 [58%] female; 380 [74%] previous non-nucleoside reverse transcriptase inhibitor exposure). Week 48 viral load was below 50 copies per mL in 246 (96%) of 255 participants in the long-acting therapy group and 250 (97%) of 257 in the oral therapy group (difference –0·8 percentage points; 95% CI –3·7 to 2·3), demonstrating non-inferiority (confirmed in per-protocol analysis). Two participants had virological failure in the long-acting therapy group, both with drug resistance; none had virological failure in the oral therapy group. Adverse events of grade 3 or greater severity occurred in 24 (9%) participants on long-acting therapy and ten (4%) on oral therapy; one participant discontinued long-acting therapy (for injection-site reaction).
Interpretation
Long-acting therapy had non-inferior efficacy compared with oral therapy, with a good safety profile, and can be considered for African treatment programmes.
Useful links
Collaborate for development
Consider on a case by case basis, collaborating on developing long acting products with potential significant public health impact, especially for low- and middle-income countries (LMICs), utilising the referred to long-acting technology
Share technical information for match-making assessment
Provide necessary technical information to a potential partner, under confidentiality agreement, to enable preliminary assessment of whether specific medicines of public health importance in LMICs might be compatible with the referred to long-acting technology to achieve a public health benefit
Work with MPP to expand access in LMICs
In the event that a product using the referred to long-acting technology is successfully developed, the technology IP holder(s) will work with the Medicines Patent Pool towards putting in place the most appropriate strategy for timely and affordable access in low and middle-income countries, including through licensing