Drug name
Last update: Jul 2026Naltrexone
Developer(s)
Drug information
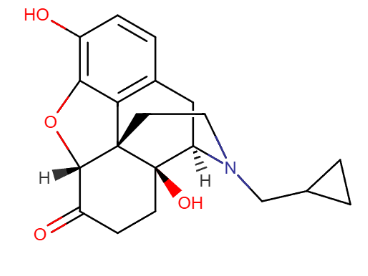
Naltrexone
VIVITROL
Small molecule
Not provided
Naltrexone long-acting injectable (LAI) is an opioid receptor antagonist with activity at μ, κ, and δ receptors, indicated for Alcohol Use Disorder and Opioid Use Disorder. VIVITROL® uses Medisorb® extended-release technology and is administered as a once-monthly intramuscular injection. An initial release occurs ~2 hours post-injection, followed by a secondary release at 2–3 days. Steady state is reached by ~14 days, with therapeutic plasma levels (>1–2 ng/mL) maintained for 28–31 days, providing continuous receptor antagonism across the dosing interval. Compared with oral naltrexone, long‑acting intramuscular naltrexone demonstrates a similar overall safety profile, while reducing risks associated with daily dosing non‑adherence.
Naltrexone 380 mg long‑acting intramuscular injection is currently approved only in the United States under the brand name VIVITROL®. Although, the company submitted Marketing Authorisation Applications (MAA) for this product in the United Kingdom and Germany on 02 April 2007.
VIVITROL® (naltrexone for extended‑release injectable suspension), 380 mg, received approval from the U.S. Food and Drug Administration on 13 April 2006.
Therapeutic area(s)
- Substance use disorders
- Treatment
Administration route
Intramuscular
Associated long-acting platforms
Polymer-based particles
Use of drug
- Administered by a community health worker
- Administered by a nurse
- Administered by a specialty health worker
- Monthly
Naltrexone Microspheres is contraindicated in: Patients receiving opioid analgesics Patients with current physiologic opioid dependence Patients in acute opioid withdrawal Any individual who has failed the naloxone challenge test or has a positive urine screen for opioids Patients who have previously exhibited hypersensitivity to naltrexone, PLG, carboxymethylcellulose, or any other components of the diluent.
Dosage
380 mg IM
380 mg every 4 weeks
The recommended dose of VIVITROL is 380 mg delivered intramuscularly (IM) as a gluteal injection, every 4 weeks or once a month, alternating buttocks for each subsequent injection, using the kit components provided in the package.
Prior to initiating VIVITROL, an opioid-free duration of a minimum of 7–10 days is recommended for patients, to avoid precipitation of opioid withdrawal that may be severe enough to require hospitalization
Associated technologies
Not provided
Comment & Information
Developer(s)

Alkermes
Alkermes plc is a Dublin-based biopharmaceutical company founded in 1987 that focuses on developing medicines for neuroscience. The company commercializes treatments for alcohol and opioid dependence (VIVITROL), schizophrenia (ARISTADA, ARISTADA INITIO), and bipolar I disorder (LYBALVI). Alkermes utilizes three primary proprietary technologies - LinkeRx, NanoCrystal, and Medisorb.
Drug structure
Scale-up and manufacturing prospects
VIVITROL is manufactured exclusively at Alkermes' facility in Wilmington, Ohio.
1. Static mixers (first and second inline mixers) 2. Positive‑displacement pumps 3. Stirred extraction vessels (primary & secondary extraction) 4. Custom vibratory sieves (25 µm & 150 µm) 5. Vacuum dryer with nitrogen bleed 6. Freezers (−20 °C) 7. Temperature‑controlled baths (5–10 °C and ambient)
Manufacturing process of Medisorb Technology based Naltrexone includes: Slow crystallization, fast crystallization, extended‑release PLGA microparticles via solvent extraction, reslurry, static mixing, drying cycles. 1. Prepare polymer solution by dissolving 75:25 DL‑PLGA in ethyl acetate (EtAc) → 16.7% w/w. 2. Solvation / crystallization in different solvents. 3. Solvate formation (ethanol, benzyl alcohol, methanol, DMF, dichloromethane, etc.). 4. Hydrate formation from water. 5. Anhydrous forms from acetonitrile crystallization. 6. Amorphous form generated by melting at 180–190 °C and quenc
XRPD (phase ID, crystallinity), Differential Scanning Calorimetry (DSC) (thermal behavior), Infrared ATR (IR‑ATR) (functional group identification) using MIRacle™ single‑reflection horizontal ATR (ZnSe)
Excipients
Not provided
1. Polylactide-co-glycolide (PLG) 2. Carboxymethylcellulose sodium salt 3. Polysorbate 20 4. Sodium chloride 5. Water for injection (WFI)
MeCl (methylene chloride), Heptane, Benzyl alcohol, Ethanol, and Ethyl acetate
Delivery device(s)
No delivery device
Publications
Saxon, A. J., Akerman, S. C., Liu, C. C., Sullivan, M. A., Silverman, B. L., & Vocci, F. J. (2018). Extended-release naltrexone (XR-NTX) for opioid use disorder in clinical practice: Vivitrol's Cost and Treatment Outcomes Registry. Addiction (Abingdon, England), 113(8), 1477–1487. https://doi.org/10.1111/add.14199
Background and aims: Extended-release naltrexone (XR-NTX), a μ-opioid receptor antagonist for prevention of relapse to opioid dependence, has demonstrated efficacy compared with placebo and comparative effectiveness with buprenorphine-naloxone. We report outcomes for XR-NTX in Vivitrol's Cost and Treatment Outcomes Registry.
Design: Observational, open-label, single-arm, multi-center registry assessing baseline characteristics and clinical and health-related quality-of-life outcomes associated with XR-NTX treatment in clinical practice.
Setting: 32 US treatment centers from 2011 to 2013.
Participants: Patients with opioid dependence who were prescribed XR-NTX treatment and then enrolled into the registry.
Measurements: Monthly visits were evaluated for the full population and for patient ubgroups retrospectively, defined by injection number, focusing on the period between baseline and month 6 (1-, 2/3- or 6-XR-NTX).
Findings: Of 403 enrolled patients, 395 were analyzed. Most patients (n = 349) received out-patient care. On average, patients received five injections (median = 3; range = 1-25). The median number of injections administered within 6 months was higher in patients who at baseline were employed (three versus two unemployed, P = 0.02) or had private insurance (five versus two self-payment, P = 0.005; versus two state-funded, P < 0.001). The 1-, 2/3- and 6-XR-NTX groups had 132, 152 and 111 patients, respectively. At baseline, the 6-XR-NTX patients were more likely to meet normal/minimal mental illness criteria and attend school and less likely to report recent drug use. Within 6 months, the 6-XR-NTX group demonstrated improvements in employment, mental health and psychosocial functioning, and decreases in opioid craving, drug use and drug-related behavior.
Conclusions: Among opioid-dependent people receiving XR-NTX treatment, better mental health, higher education and lower recent drug use at baseline are associated with greater treatment duration; in turn, longer treatment duration is associated with lower relapse rates and improved outcomes generally.
Keywords: Extended-release naltrexone; Vivitrol; medication assisted treatment; opioid dependence; opioid use disorder; registry.
Sullivan, M. A., Bisaga, A., Pavlicova, M., Carpenter, K. M., Choi, C. J., Mishlen, K., Levin, F. R., Mariani, J. J., & Nunes, E. V. (2019). A Randomized Trial Comparing Extended-Release Injectable Suspension and Oral Naltrexone, Both Combined With Behavioral Therapy, for the Treatment of Opioid Use Disorder. The American journal of psychiatry, 176(2), 129–137. https://doi.org/10.1176/appi.ajp.2018.17070732
Objective:
The oral formulation of the opioid antagonist naltrexone has shown limited effectiveness for treatment of opioid use disorder due to poor adherence. Long-acting injection naltrexone (XR-naltrexone), administered monthly, circumvents the need for daily pill taking, potentially improving adherence, and has been shown to be superior to placebo in reducing opioid use over 6 months of treatment. This open-label trial compared the outcomes of patients with opioid use disorder treated with XR-naltrexone or oral naltrexone in combination with behavioral therapy.
Method:
Sixty opioid-dependent adults completed inpatient opioid withdrawal and were transitioned to oral naltrexone. They were stratified by severity of opioid use (six or fewer bags versus more than six bags of heroin per day) and randomly assigned (1:1) to continue treatment with oral naltrexone (N=32) or XR-naltrexone (N=28) for 24 weeks. The first dose of XR-naltrexone (380 mg) was administered prior to discharge, with monthly doses thereafter, and oral naltrexone was given in a 50-mg daily dose. All participants received weekly behavioral therapy to support treatment and adherence to naltrexone.
Results:
A Cox proportional hazards model adjusting for race, gender, route of use, and baseline opioid use severity indicated that significantly more patients were retained in treatment for 6 months in the XR-naltrexone group (16 of 28 patients, 57.1%) than in the oral naltrexone group (nine of 32 patients, 28.1%) (hazard ratio=2.18, 95% CI=1.07, 4.43).
Conclusions:
Patients receiving XR-naltrexone had twice the rate of treatment retention at 6 months compared with those taking oral naltrexone. These results support the use of XR-naltrexone combined with behavioral therapy as an effective treatment for patients seeking opioid withdrawal and nonagonist treatment for preventing relapse to opioid use disorder.
Additional documents
No documents were uploaded
Useful links
There are no additional links
Collaborate for development
Consider on a case by case basis, collaborating on developing long acting products with potential significant public health impact, especially for low- and middle-income countries (LMICs), utilising the referred to long-acting technology
Share technical information for match-making assessment
Provide necessary technical information to a potential partner, under confidentiality agreement, to enable preliminary assessment of whether specific medicines of public health importance in LMICs might be compatible with the referred to long-acting technology to achieve a public health benefit
Work with MPP to expand access in LMICs
In the event that a product using the referred to long-acting technology is successfully developed, the technology IP holder(s) will work with the Medicines Patent Pool towards putting in place the most appropriate strategy for timely and affordable access in low and middle-income countries, including through licensing