Drug name
Last update: Jul 2026Gemcitabine Intravesical LAI
Developer(s)
Drug information
Gemcitabine
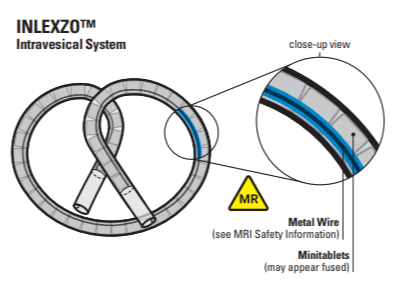
INLEXZO
Small molecule
Not provided
Gemcitabine (INLEXZO) is a nucleoside metabolic inhibitor-containing intravesical system, indicated for the treatment of adult patients with Bacillus Calmette-Guérin (BCG)-unresponsive, non-muscle invasive bladder cancer (NMIBC) with carcinoma in situ (CIS) with or without papillary tumors. Gemcitabine in-situ is metabolized by nucleoside kinases to diphosphate (dFdCDP) and triphosphate (dFdCTP) nucleosides. Thus, the plasma gemcitabine remains below quantification, and plasma 2′,2′-Difluorodeoxyuridine appears only at very low levels. High urinary concentrations persist through the indwelling period, with 77% excreted by Day 7 and 99% by Day 21. Bladder tissue studies show sustained penetration of active metabolites for up to 96 hours, achieving high local exposure with low systemic risk.
INLEXZO (gemcitabine intravesical system) has been approved in United States of America on 09 September 2025. This product received Breakthrough Therapy Designation from USFDA in 2023.
Gemcitabine Intravesical System (INLEZXO) 225 mg is approved by USFDA only.
Therapeutic area(s)
- Oncology : "Bacillus Calmette-Guérin (BCG)-unresponsive, non-muscle invasive bladder cancer (NMIBC) with carcinoma in situ (CIS) with or without papillary tumors"
- Treatment
Administration route
Intravesical
Associated long-acting platforms
bi-oval-shaped osmotic urinary catheter based delivery system
Use of drug
- Administered by a community health worker
- Administered by a nurse
- Administered by a specialty health worker
- Every 3 months
- Every 3 weeks
Common side effects include Frequent urination, dysuria (painful urination), and micturition urgency. INLEXZO is contraindicated in patients with a perforated bladder. Administration in such cases can lead to severe systemic exposure to Gemcitabine. Systemic exposure may cause fetal harm. Females of reproductive potential should use effective contraception during treatment and for 6 months following final removal. Males with partners of reproductive potential should use effective contraception during treatment and for 3 months following final removal.
Dosage
225 mg every 3 weeks
225 mg
Gemcitabine Intravesical System (225 mg of gemcitabine) into the bladder once every 3 weeks for up to 6 months (8 doses), followed by once every 12 weeks for up to 18 months (6 doses), or until persistent or recurrent NMIBC, disease progression, or unacceptable toxicity.
Not provided
Associated technologies
Not provided
Comment & Information
Developer(s)

Johnson & Johnson
Janssen Biotech, Inc. is a leading biotechnology subsidiary of Johnson & Johnson (J&J) that specializes in developing, manufacturing, and commercializing therapeutic products to treat serious medical conditions. As of 2026, the company is part of the Johnson & Johnson Innovative Medicine division, following a global rebranding initiative to unite J&J's pharmaceutical segments under a single brand
Drug structure
Scale-up and manufacturing prospects
Projected revenue for INLEXZO is expected to reach $33 million in 2025 and increase significantly to $223 million in 2026.
Tablet equipments: 1. Precision analytical balances / weigh booths 2. Powder blender / tumble mixer 3. Mini‑tablet press 4. Controlled‑humidity storage cabinets Polymer Component Fabrication Equipment: 1. Medical‑grade silicone extrusion line 2. Hydrophilic TPU film extrusion / casting machines 3. Precision die‑cutters 4. Laser micromachining system 5. Nitinol wire forming and heat‑setting furnace
Process include (ISO‑classified cleanrooms required: Tablet handling/assembly: ISO 7–8; Device loading / open processes: ISO 5–7): 1. Mini‑Tablet Drug Core Production 2. Polymer Component Fabrication 3. Device Assembly 4. Sterilization & Packaging 5. In‑Vitro Release Testing (QC Lot Release)
1. HPLC‑UV 2. LC‑MS 3. Durometer tester, tensile tester, microscopy, contact‑angle/swelling measurement 4. Bioburden test kit
Excipients
No proprietary excipient used
1. Polyethylene glycol 8000 (8.0 mg) 2. Povidone K30 (13.4 mg) 3. Urea (42.6 mg) in a single intravesical implantable system
Not provided
Delivery device(s)
intravesical implantable device containing solid gemcitabine tablets
Drug delivery device, for bladder delivery of 75% w/w gemcitabine HC1)
Implantable drug delivery devices include a housing defining a reservoir, a first unit within the reservoir, and a second unit within the reservoir. The first unit contains a drug and the second unit contains a functional agent that facilitates release of the drug. Intravesical drug delivery devices include a housing portion containing a drug formulation and a housing portion containing an excipient, and are configured to release the drug according to a first release profile and the excipient according to a second release profile.
WO2015026813
Device
WO2015026813
Not provided
August 19, 2034
Granted: AU, BR, CA, CN, EP (AL, AT, BE, BG, CH, CY, CZ, DE, DK, EE, ES, FI, FR, GB, GR, HR, HU, IE, IS, IT, LI, LT, LU, LV, MC, MK, MT, NL, NO, PL, PT, RO, RS, SE, SI, SK, SM, TR), IL, IN, JP, KR, MX, NZ, RU, SG, US, VN, ZA
Drug delivery device wholly deployable within the bladder
Intravesical devices are provided that are wholly deployable within the bladder of a patient in need of treatment and are well tolerated by the patient.
WO2011084712
Device
TARIS BIOMEDICAL LLC
Not provided
December 17, 2030
Granted: AU, CA, EP (AL, AT, BE, BG, CH, CY, CZ, DE, DK, EE, ES, FI, FR, GB, GR, HR, HU, IE, IS, IT, LI, LT, LU, LV, MC, MK, MT, NL, NO, PL, PT, RO, RS, SE, SI, SK, SM, TR), JP, US Pending: IL
Drug delivery device and drug tablet comprising a local anaesthetic agent
A drug delivery device is provided that includes a device body, a number of solid, compressed drug tablets, and a retention frame. The device body includes a drug reservoir lumen and a retention frame lumen. The number of solid, compressed drug tablets are positioned in the drug reservoir lumen, and the retention frame is positioned in the retention frame lumen. The drug tablets may be mini-tablets aligned in the drug reservoir lumen, with an interstice formed between any two adjacent drug tablets facilitating deformation of the device body. Systems and method are also provided for loading a drug delivery device.
WO2010151893, WO2010151896
Device
TARIS BIOMEDICAL LLC
Not provided
June 28, 2030
Granted: CA, CN, EP (CH, DE, FR, GB, IE, DK, FI, HU, NL, SE, ES, IT), EA (KZ, RU), IN, IL, JP, KR, MX, US Pending: AU, BR Not in force: EG, NZ, PH, SG, ZA, VN
Gemcitabine compound
This invention belongs to the field of pharmaceutical chemistry, and provides a new difluoro carbohydrate and new antiviral nucleosides prepared by coupling the new carbohydrate with appropriate bases.
US4808614
Compound
Eli Lilly and Company
Not provided
May 5, 2010
Expired
Publications
Tyson MD, Morris D, Palou J, Rodriguez O, Mir MC, Dickstein RJ, Guerrero-Ramos F, Scarpato KR, Hafron JM, Messing EM, Cutie CJ, Maffeo JC, Raybold B, Chau A, Stromberg KA, Keegan KA. Safety, Tolerability, and Preliminary Efficacy of TAR-200 in Patients With Muscle-invasive Bladder Cancer Who Refused or Were Unfit for Curative-intent Therapy: A Phase 1 Study. J Urol. 2023 May;209(5):890-900. doi: 10.1097/JU.0000000000003195. Epub 2023 Apr 7. PMID: 37026631; PMCID: PMC12721624.
Purpose: Half of patients with muscle-invasive bladder cancer worldwide may not receive curative-intent therapy. Elderly or frail patients are most affected by this unmet need. TAR-200 is a novel, intravesical drug delivery system that provides sustained, local release of gemcitabine into the bladder over a 21-day dosing cycle. The phase 1 TAR-200-103 study evaluated the safety, tolerability, and preliminary efficacy of TAR-200 in patients with muscle-invasive bladder cancer who either refused or were unfit for curative-intent therapy.
Materials and methods: Eligible patients had cT2-cT3bN0M0 urothelial carcinoma of the bladder. TAR-200 was inserted for 4 consecutive 21-day cycles over 84 days. The primary end points were safety and tolerability at 84 days. Secondary end points included rates of clinical complete response and partial response as determined by cystoscopy, biopsy, and imaging; duration of response; and overall survival.
Results: Median age of the 35 enrolled patients was 84 years, and most were male (24/35, 68.6%). Treatment-emergent adverse events related to TAR-200 occurred in 15 patients. Two patients experienced treatment-emergent adverse events leading to removal of TAR-200. At 3 months, complete response and partial response rates were 31.4% (11/35) and 8.6% (3/35), respectively, yielding an overall response rate of 40.0% (14/35; 95% CI 23.9-57.9). Median overall survival and duration of response were 27.3 months (95% CI 10.1-not estimable) and 14 months (95% CI 10.6-22.7), respectively. Progression-free rate at 12 months was 70.5%.
Conclusions: TAR-200 was generally safe, well tolerated, and had beneficial preliminary efficacy in this elderly and frail cohort with limited treatment options.
Pradere B, Schuit M, Guerrero-Ramos F, Shariat SF, Kitamura H, Jacob JM, Bao Y, Heesakkers J, Peters KM, Cahn DJ, De Troyer B, Herrera Imbroda B, Morris DS, Pieczonka CM, Wei Q, Bhanvadia S, Somer R, Jessner W, Triantos S, Sánchez de Llano C, Maffeo JC, Sweiti H, Psutka SP. Side effect management and procedural best practices with indwelling intravesical drug-releasing systems in the treatment of bladder cancer: recommendations from expert panels. Curr Opin Urol. 2025 Oct 8;36(1):123–33. doi: 10.1097/MOU.0000000000001350. Epub ahead of print. PMID: 41065373; PMCID: PMC12700673.
Purpose of review
To provide expert recommendations for side effect management in patients with bladder cancer receiving intravesical-drug releasing system (iDRS) treatment and for optimizing iDRS insertion procedure success.
Recent findings
Indwelling iDRS are designed to provide sustained local exposure to therapy. In clinical trials, frequent side effects of iDRS treatment were lower urinary tract symptoms (LUTS) (e.g., dysuria, pollakiuria, micturition urgency), urinary tract infections (UTIs), and hematuria. These side effects are generally low grade, but if not properly managed, may lead to treatment interruptions or discontinuations. As data are limited, practical recommendations based on expert opinion for the management of common side effects and best practices for iDRS insertion procedures may improve treatment adherence and optimize outcomes in patients with bladder cancer receiving iDRS.
Summary
Two separate expert panels were convened to develop recommendations for side effect management with iDRS and optimizing iDRS insertion procedure success. Stepwise treatment-specific management strategies for LUTS, UTIs, and hematuria in patients receiving iDRS treatment that are familiar to practicing urologists are presented, including considerations for continuation or discontinuation of iDRS treatment. Several advanced techniques can be considered to improve iDRS insertions based on variations in patient anatomy.
Daneshmand, S., Brummelhuis, I. S. G., Pohar, K. S., Steinberg, G. D., Aron, M., Cutie, C. J., Keegan, K. A., Maffeo, J. C., Reynolds, D. L., Raybold, B., Chau, A., & Witjes, J. A. (2022). The safety, tolerability, and efficacy of a neoadjuvant gemcitabine intravesical drug delivery system (TAR-200) in muscle-invasive bladder cancer patients: a phase I trial. Urologic oncology, 40(7), 344.e1–344.e9. https://doi.org/10.1016/j.urolonc.2022.02.009
Objectives: Neoadjuvant chemotherapy and radical cystectomy (RC) are underutilized standards of care for the treatment of muscle-invasive bladder cancer (MIBC) due to high patient burden from systemic toxicities and postoperative complications, respectively. TAR-200 is a novel intravesical drug delivery system developed to release gemcitabine into the bladder urine continuously, resulting in distribution of drug into stromal layers of the bladder. The primary aim of the TAR-200-101 study was to evaluate the safety of TAR-200 in patients with MIBC prior to RC (NCT02722538).
Methods and materials: This phase I, open-label study was conducted across 6 US and European sites. Eligible patients were aged ≥18 years with histologically confirmed T2a-T3b N0-N1 M0 urothelial cancer and had refusal or were ineligible to receive cisplatin-based combination chemotherapy. Two arms were enrolled serially. Patients in Arm 1 had residual tumor >3 cm after transurethral resection of bladder tumor (TURBT); those in Arm 2 had undergone maximal TURBT (residual tumor <3 cm). Patients received two 7-day cycles of intravesical gemcitabine delivery via TAR-200 before undergoing RC. Primary outcome was safety; secondary outcomes were tolerability, pharmacokinetics, and preliminary efficacy.
Results: Of 23 patients in the intention-to-treat population (11 in Arm 1, 12 in Arm 2), 20 completed both dosing cycles of TAR-200. No patients were classified as intolerant to TAR-200. Ten patients (4 in Arm 1, 6 in Arm 2) experienced ≥1 treatment-emergent adverse events (TEAEs). The most common TAR-200-related TEAEs were pollakiuria (n = 3) and urinary incontinence (n = 2). All TEAEs prior to RC were grade ≤2; 1 patient in Arm 2 experienced a grade 3 non-treatment-related TEAE. Plasma gemcitabine levels were undetectable. In Arm 1, those with residual tumor, 4 of 10 patients exhibited pathologic downstaging; 1 experienced a complete response (CR) and 3 a partial response (PR). In Arm 2, those undergoing maximal TURBT, 6 of 10 patients exhibited downstaging; 3 experienced a CR and 3 a PR.
Conclusion: Controlled intravesical gemcitabine release via TAR-200 was safe and well tolerated in patients with MIBC.
Additional documents
No documents were uploaded
Useful links
Collaborate for development
Consider on a case by case basis, collaborating on developing long acting products with potential significant public health impact, especially for low- and middle-income countries (LMICs), utilising the referred to long-acting technology
Share technical information for match-making assessment
Provide necessary technical information to a potential partner, under confidentiality agreement, to enable preliminary assessment of whether specific medicines of public health importance in LMICs might be compatible with the referred to long-acting technology to achieve a public health benefit
Work with MPP to expand access in LMICs
In the event that a product using the referred to long-acting technology is successfully developed, the technology IP holder(s) will work with the Medicines Patent Pool towards putting in place the most appropriate strategy for timely and affordable access in low and middle-income countries, including through licensing