Technology name
Last update: Mar 2026Multi-Arm Polymer Conjugated Immmunotherapies
Developer(s)
Sponsor(s)
Not specified
Type of technology
Polymer-based particles
Administration route
Intratumoral, Intravenous
Development state and regulatory approval
Antineoplastic and immunomodulating agents
Phase II
Not approved yet
Description
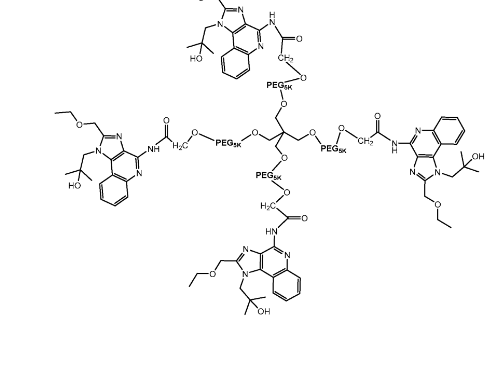
This technology uses multi‑arm polymer conjugates of TLR7/8 agonists to activate local antitumor immunity while minimizing systemic toxicity. Delivered intratumorally, these conjugates stay in the tumor, enhance antigen presentation, and boost CD8⁺ T‑cell responses. The release of the TLR7/8 agonist from the polymer conjugate depends on the linkage‑containing spacer (Xₐ) connecting the polymer (POLY) to the drug. When combined with a long‑acting IL‑2Rβ‑biased agonist, they produce synergistic, systemic antitumor effects and strong abscopal responses.
Developer(s)

Nektar Therapeutics
Nektar Therapeutics (Nasdaq: NKTR) is a clinical-stage biopharmaceutical company headquartered in San Francisco, California. Founded in 1990, the company specializes in immunotherapy, utilizing proprietary PEGylation and polymer conjugate technology platforms to develop drug candidates for autoimmune disorders, chronic inflammation, and oncology.
Technology highlight
1. Core Scaffold (R) – Polyol / Polythiol / Polyamine Backbone (Eg: pentaerythritol, glycerol, trimethylolpropane, polyglycerols) 2. Linker Atom (Oxygen (O), Sulfur (S), Nitrogen (–NH–)) 3. Polymer Arms (Polyethylene glycol 2,000–150,000 Da) 4. Linkage‑Containing Spacer (Xᵣ) 5. API
Illustration(s)
Technology main components
The conjugated complex has 1. Core Scaffold (R) – Polyol / Polythiol / Polyamine Backbone (Eg: pentaerythritol, glycerol, trimethylolpropane, polyglycerols) 2. Linker Atom (Oxygen (O), Sulfur (S), Nitrogen (–NH–)) 3. Polymer Arms (Polyethylene glycol 2,000–150,000 Da) 4. Linkage‑Containing Spacer (Xᵣ) 5. API
Not provided
Delivery device(s)
No delivery device
APIs compatibility profile
Unit: mg/mL
(i) Antiviral agents (particularly HIV and chronic viral infections) Nucleos(t)ide reverse transcriptase inhibitors (NRTIs), Non-nucleoside reverse transcriptase inhibitors (NNRTIs) Integrase strand transfer inhibitors (INSTIs), Protease inhibitors; (ii) Antibacterial agents (including TB and chronic bacterial infections) Rifamycins, Macrolides, Fluoroquinolones; (iii) Antifungal agents; (iv) Antiparasitic agents; (v) Anti-inflammatory and immunomodulatory drugs; (vi) Anticancer agents and (vii) CNS-active drugs (viii) TLR 7/8 agonists N-[4-(4-amino-2- ethyl-1H-imidazo[4,5c]quinolin-1-yl)butyl
Rezpegaldesleukin and Bempegaldesleukin
Not provided
Not provided
75-90 wt%
1 single API :
Min: 1.5 Max: 6.5
Scale-up and manufacturing prospects
Not provided
1. Reaction Vessels/bioreactors 2. Magnetic stirrers 3. Heating plates / heating mantles 4. Cooling baths (20°C, 50°C, 60°C operations described) 5. Temperature controllers / thermometers 6. Hand‑swirling for dissolution 7. Nitrogen/argon inert atmosphere setups (implied by anhydrous conditions) 8. Filtration apparatus (frit funnels, Büchner funnels) 9. Vacuum filtration setups 10. High‑vacuum drying systems (overnight drying)
To manufacture multi-arm conjugated complex, we need ISO cleanroom (class not explicited mentioned). Step1: Derive polymer from Lactide, Glycolide, Caprolactone or Combinations thereof (copolymers) Step 2: Ring-opening polymerization - initiated by alcohol-based initiators, using metal-based catalysts (e.g., tin-based catalysts) Step 3: Polymer purification, Removal of unreacted monomer, Drying of the polymer prior to formulation use Step 4: API and Polymer complex formation using Melt or semi-solid processing or solvent based mixing.
1. 500 MHz Bruker ¹H NMR spectrometer Drug content & release: 2. HPLC or UPLC 3. UV–Vis spectroscopy Polymer–drug interaction: 4. DSC (thermal behavior) 5. FTIR (compatibility assessment) Physical characterization: 6. Particle size analyzers (if particulate) 7. Microscopy (optical / SEM implied) Stability & performance: 8. Dissolution or release testing apparatus 9. Accelerated stability chambers
Excipients
Not provided
1. Carbohydrates (Monosaccharides; Disaccharides; Polysaccharides; Sugar alcohols (Alditols)) 2. Inorganic Salts (NaCl; KCl; NaSO4; KNO3; Na2PO3/Na2PO4) 3. Antimicrobial Agents (Benzalkonium chloride, Benzethonium chloride, Benzyl alcohol) 4. Antioxidants (Butylated hydroxyanisole (BHA)) 5. Surfactants (Polysorbates, Pluronics) 6. Buffers (Phosphate buffers) 7. Acids (HCL. HPO3, Acetic acid and citric acid) 8. Bases (NaOH, KOH, NH3OH)
Not provided
Additional features
- Biodegradable
The release kinetics of the active pharmaceutical ingredient (API) are influenced by multiple factors, including the chemical stability of the linker (with ester < carbonate < carbamate < amide), local pH conditions, and the presence and activity of relevant enzymes (e.g., esterases and proteases). Additional determinants include PEG arm length and molecular architecture, as well as the degree of drug loading, defined by the number of conjugated arms.
This technology is adminstered as intratumoral injection. Intratumoral administration is conducted using a fine-gauge needle (approximately 22–25 gauge), with needle insertion angle and depth selected based on tumor size, location, and imaging guidance, where applicable.
Rezpegaldesleukin (NKTR-358; REZPEG) is a polyethylene glycol–conjugated recombinant human interleukin-2 (rhIL-2). Phase 2 results show Treatment-emergent adverse events (TEAEs) were reported in 66.0% of subjects receiving REZPEG compared with 48.7% of those receiving placebo, while treatment-related adverse events (TRAEs) occurred in 41.9% and 10.4% of subjects, respectively. Severe TEAEs were reported in 3.2% of subjects in the REZPEG group and 4.5% in the placebo group. The most frequently reported TRAE with REZPEG was injection-site reaction (ISR), occurring in 26.4% of subjects.
- In situ stability: The stability of the conjugate in circulation is influenced by linker chemistry. Stable linkers (e.g., amides, thioethers) are resistant to hydrolytic cleavage under physiological conditions, whereas releasable linkers undergo gradual cleavage in biological environments. PEG chains (e.g., PEG 20 kDa) enhance aqueous solubility and reduce the risk of drug precipitation. -Formulation stability: Long-term stability studies are typically conducted under controlled conditions (25 °C ± 2 °C / 60% RH ± 5% RH). but no results were disclosed.
1. Refrigeration at 2–8 °C (most PEGylated cytokines) 2. Temperature‑controlled shipping
Therapeutic area(s)
- Diabetes
- Other(s) : "dermatological disorders like alopecia areata and acute dermatitis and scarring disorders"
- HIV
- Oncology : "Solid Tumors and Large B-Cell Lymphoma"
- Treatment
Potential associated API(s)
- Antineoplastic and immunomodulating agents
- Antineoplastic and immunomodulating agents
- Antineoplastic and immunomodulating agents
- Antineoplastic and immunomodulating agents
- Antineoplastic and immunomodulating agents
- Antineoplastic and immunomodulating agents
Use of technology
- Administered by a community health worker
- Administered by a nurse
- Administered by a specialty health worker
Monthly, Every 2 weeks, Every 3 weeks
Not provided
Targeted user groups
- Adults
- Older Adults
- All
Unspecified
Unspecified
Unspecified
Not provided
Antineoplastic and immunomodulating agents
IL-2 receptor agonist
Phase II
NCT06136741
Diabetes mellitus type 2 (T2DM), Acute dermatitis and Alopecia Areata
Not provided
Every 2 weeks
Not approved yet
Antineoplastic and immunomodulating agents
Tumor necrosis factor receptor 2 agonist (TNFR2)
Pre-clinical
Not provided
Ulcerative Colitis, Vitiligo, Multiple Sclerosis
Not provided
Not provided
Not approved yet
Antineoplastic and immunomodulating agents
Bispecific antibody incorporating TNFR agonist
Pre-clinical
Not provided
Autoimmune Diseases
Not provided
Not provided
Not approved yet
Antineoplastic and immunomodulating agents
Colony stimulating factor 1 (CSF-1)
Pre-clinical
Not provided
Fibrotic diseases
Not provided
Not provided
Not approved yet
Antineoplastic and immunomodulating agents
IL-15 receptor agonist
Phase II
NCT04136756
Solid Tumors and Large B-Cell Lymphoma (Relapsed/Refractory Multiple Myeloma & Non-Hodgkin Lymphoma)
Not provided
Every 3 weeks, every 4 weeks IV infusion
Not approved yet
Antineoplastic and immunomodulating agents
IL-2 receptor agonist
Phase II
NCT03138889
Locally Advanced or Metastatic Solid Tumors
Not provided
Every 3 weeks
Not approved yet
Multi-arm polymer conjugates of tlr agonist compounds and related immunotherapeutic treatment methods
Provided are multi-arm polymer conjugates of Toll-Like Receptor ("TLR") agonists such as TLR 7/8 agonists, as well as related compositions, and methods of making and using such conjugates. Exemplary conjugates are encompassed by Formula I: (I) or a pharmaceutically acceptable salt form thereof, where R, taken together with each Q, is a residue of a polyol, polythiol, or polyamine bearing from 3 to about 50 hydroxyl, thiol, or amino groups; each Q is a linker selected from oxygen, sulfur and -NH; each POLY is independently a water-soluble, non-peptidic polymer; each Xr is independently a linkage-containing spacer moiety; q is a positive integer from 3 to about 50; and each TLR 7/8 AG is a Toll-like receptor 7/8 agonist. Also provided is a method of administering to a patient having cancer.
WO2018132496A1
Not provided
Nektar Therapeutics
Not provided
October 17, 2019
Ceased
Publications
Silverberg JI, Rosmarin D, Chovatiya R, Bieber T, Schleicher S, Beck L, Gooderham M, Chaudhry S, Fanton C, Yu D, Levy J, Liu Y, Miyazaki T, Tagliaferri M, Schmitz C, Nirula A, Kotzin B, Zalevsky J. The regulatory T cell-selective interleukin-2 receptor agonist rezpegaldesleukin in the treatment of inflammatory skin diseases: two randomized, double-blind, placebo-controlled phase 1b trials. Nat Commun. 2024 Oct 25;15(1):9230. doi: 10.1038/s41467-024-53384-1. PMID: 39455575; PMCID: PMC11511931.
Regulatory T cell (Treg) impairment is implicated in the pathogenesis of chronic inflammatory diseases, but relatively little is known about the therapeutic potential of Treg restoration. Here we present clinical evidence for the Treg-selective interleukin-2 receptor agonist rezpegaldesleukin (REZPEG) in two randomized, double-blind, placebo-controlled Phase 1b trials in patients with moderate-to-severe atopic dermatitis (AD) (NCT04081350) or chronic plaque psoriasis (PsO) (NCT04119557). Key inclusion criteria for AD included an Eczema Area and Severity Index (EASI) score ≥ 16 and a validated Investigator Global Assessment for Atopic Dermatitis (vIGA-AD) ≥ 3, and for PsO included a Psoriasis Area and Severity Index (PASI) score of ≥ 12 and a static Physician's Global Assessment (sPGA) score of ≥ 3. REZPEG is safe and well-tolerated and demonstrates consistent pharmacokinetics in participants receiving subcutaneous doses of 10 to 12 µg/kg or 24 µg/kg once every 2 weeks for 12 weeks, meeting the primary and secondary objectives, respectively. AD patients receiving the higher dose demonstrate an 83% improvement in EASI score after 12 weeks of treatment. EASI improvement of ≥ 75% (EASI-75) and vIGA-AD responses are maintained for 36 weeks after treatment discontinuation in 71% and 80% of week 12 responders, respectively. These exploratory clinical improvements are accompanied by sustained increases in CD25bright Tregs. REZPEG thus represents a homeostatic approach to cutaneous disease therapy and holds clinical potential in providing long-term, treatment-free disease control.
Charych DH, Hoch U, Langowski JL, Lee SR, Addepalli MK, Kirk PB, Sheng D, Liu X, Sims PW, VanderVeen LA, Ali CF, Chang TK, Konakova M, Pena RL, Kanhere RS, Kirksey YM, Ji C, Wang Y, Huang J, Sweeney TD, Kantak SS, Doberstein SK. NKTR-214, an Engineered Cytokine with Biased IL2 Receptor Binding, Increased Tumor Exposure, and Marked Efficacy in Mouse Tumor Models. Clin Cancer Res. 2016 Feb 1;22(3):680-90. doi: 10.1158/1078-0432.CCR-15-1631. PMID: 26832745.
Purpose: Aldesleukin, recombinant human IL2, is an effective immunotherapy for metastatic melanoma and renal cancer, with durable responses in approximately 10% of patients; however, severe side effects limit maximal dosing and thus the number of patients able to receive treatment and potential cure. NKTR-214 is a prodrug of conjugated IL2, retaining the same amino acid sequence as aldesleukin. The IL2 core is conjugated to 6 releasable polyethylene glycol (PEG) chains. In vivo, the PEG chains slowly release to generate active IL2 conjugates.
Experimental design: We evaluated the bioactivity and receptor binding of NKTR-214 and its active IL2 conjugates in vitro; the tumor immunology, tumor pharmacokinetics, and efficacy of NKTR-214 as a single agent and in combination with anti-CTLA-4 antibody in murine tumor models. Tolerability was evaluated in non-human primates.
Results: In a murine melanoma tumor model, the ratio of tumor-killing CD8(+) T cells to Foxp3(+) regulatory T cells was greater than 400 for NKTR-214 compared with 18 for aldesleukin, supporting preferential activation of the IL2 receptor beta over IL2 receptor alpha, due to the location of PEG molecules. NKTR-214 provides a 500-fold greater exposure of the tumor to conjugated IL2 compared with aldesleukin. NKTR-214 showed efficacy as a single agent and provided durable immunity that was resistant to tumor rechallenge in combination with anti-CTLA-4 antibody. NKTR-214 was well tolerated in non-human primates.
Conclusions: These data support further evaluation of NKTR-214 in humans for a variety of tumor types, adding to the repertoire of potent and potentially curative cancer immunotherapies.
Additional documents
No documents were uploaded
Useful links
There are no additional links
Collaborate for development
Consider on a case by case basis, collaborating on developing long acting products with potential significant public health impact, especially for low- and middle-income countries (LMICs), utilising the referred to long-acting technology
Share technical information for match-making assessment
Provide necessary technical information to a potential partner, under confidentiality agreement, to enable preliminary assessment of whether specific medicines of public health importance in LMICs might be compatible with the referred to long-acting technology to achieve a public health benefit
Work with MPP to expand access in LMICs
In the event that a product using the referred to long-acting technology is successfully developed, the technology IP holder(s) will work with the Medicines Patent Pool towards putting in place the most appropriate strategy for timely and affordable access in low and middle-income countries, including through licensing






All sponsors
No sponsor indicated