Drug name
Last update: Jul 2026Semaglutide
Developer(s)
Drug information
Semaglutide
OZEMPIC; RYLEBUS; and WEGOVY
Biotherapeutic
GLP-1 receptor agonist
Semaglutide LAI is a once-weekly subcutaneous GLP-1 receptor agonist (94% homologous to human GLP-1) indicated for glycemic control in type 2 diabetes. It enhances glucose-dependent insulin secretion, suppresses glucagon, and delays gastric emptying, lowering glucose and promoting weight loss. Peak plasma concentration occurs 1–3 days post-dose; high albumin binding confers a ~7-day half-life. Apparent clearance is ~0.05 L/h, and steady state is reached in 4–5 weeks. Furthermore, phase 3 trials show ~1.5% HbA1c reduction and up to 15% weight loss. To add on, semaglutide LAI has a black box warning i.e. risk of thyroid c-cell tumor. Other Adverse events include pancreatitis, diabetic retinopathy, hypoglycemia, acute kidney injury, and acute gallbladder diseases.
Ozempic (2 mg/3 mL, 4 mg/3 mL, and 8 mg/3 mL prefilled syringes) is approved in 54 countries, while Wegovy (0.25 mg, 0.5 mg, 1 mg, 1.7 mg, and 2.4 mg) is approved in 43 countries. Additionally, a biosimilar version of long-acting semaglutide injection, marketed as Semavic Next, is approved in the Russian Federation for the treatment of obesity.
Semaglutide has received regulatory approval in 96 countries, including authorizations from major agencies such as the U.S. Food and Drug Administration (FDA), European Medicines Agency (EMA), Pharmaceuticals and Medical Devices Agency (PMDA, Japan), Therapeutic Goods Administration (TGA, Australia), Health Canada, and Medsafe (New Zealand). The long-acting injectable (LAI) formulation of semaglutide is approved for the treatment of both type 2 diabetes mellitus and obesity/overweight, with indications and dosing regimens varying by therapeutic use.
Therapeutic area(s)
- Diabetes : "Type 2"
- Obesity / Weight Management
- Treatment
Administration route
Subcutaneous
Associated long-acting platforms
Aqueous drug particle suspension
Use of drug
- Administered by a community health worker
- Administered by a nurse
- Administered by a specialty health worker
- Self-administered
- Weekly
1. Safety and efficacy of OZEMPIC have not been established in pediatric patients (younger than 18 years). 2. No dose adjustment needed for hepatic or renal impairment.
Dosage
OZEMPIC: 2mg/3mL (0.68mg/mL); 4mg/3mL (1.34 mg/mL) & 8mg/3mL (2.68mg/mL) and WEGOVY: 0.25 mg / 0.5 mL; 0.5 mg / 0.5 mL; 1 mg / 0.5 mL ; 1.7 mg / 0.75 mL & 2.4 mg / 0.75 mL
OZEMPIC 2 mg once a week; WEGOVY 2.4 mg once a week
Start at Semaglutide 0.25 mg SC once weekly injection (with/without meals). After 4 weeks, increase the dose to 0.5 mg once weekly. If after at least 4 weeks additional glycemic control is needed, increase to 1 mg once weekly
1. OZEMPIC is approved for adults with type 2 diabetes mellitus (≥ 18 years old). 2. WEGOVY is approved for adults and adolescents aged < 12 years and older. 3. Not recommended as first-line therapy for patients inadequately controlled on diet and exercise. 4. Has not been studied in patients with a history of pancreatitis. Consider another antidiabetic therapy. 5. Not indicated for use in type 1 diabetes mellitus or treatment of diabetic ketoacidosis.
Comment & Information
Developer(s)

Novo Nordisk
Novo Nordisk A/S, founded in 1989 through the merger of two Danish insulin pioneers—Nordisk Insulinlaboratorium (1923) and Novo Terapeutisk Laboratorium (1925)—traces its roots to Nobel laureate August Krogh’s efforts to bring insulin production to Denmark. Headquartered in Bagsværd, Denmark, the company operates production facilities in nine countries and offices in over 75.
Various generic manufacturersVarious generic manufacturers
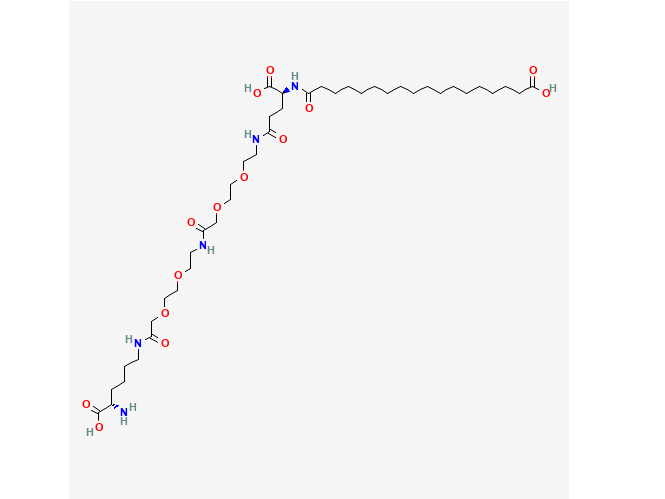
Drug structure
Scale-up and manufacturing prospects
The semaglutide LAI market is projected to grow from $28.4 billion in 2024 to $93.6 billion by 2035, at a CAGR (Compound Annual Growth Rate) of ~10.5%
1. Solid-phase peptide synthesizer (e.g., Merrifield-type) 2. Reagents for Fmoc or t-Boc chemistry 3. Protective group handling systems 4. Bioreactors 5. Fermentation tanks 6. Lyophilizers (freeze-drying) 7. Spray dryers (optional) 8. Sterile mixing tanks for aqueous formulations 9. Automated purification systems (HPLC)
Semaglutide LAI synthesis involves peptide chain assembly via solid-phase synthesis, cleavage, purification (HPLC), and lyophilization. Manufacturing requires ISO Class 7 cleanrooms, strict temperature/humidity control, and aseptic fill-finish areas. Facilities must meet cGMP and FDA/EMA standards, with HEPA filtration, stainless steel surfaces, and validated HVAC systems. Process includes: 1. Peptide Backbone synthesis 2. Non natural amino acids incorporation 3. Albumin binding moiety attachment (acylation) 4. Purification 5. Final Formulation preparation
1. UPLC/HPLC systems (for purity and stability) 2. MALDI-TOF mass spectrometer 3. ELISA and LOCI assay kits (for potency and plasma concentration) 4. AlphaScreen cAMP assay system 5. LC-MS systems (for pharmacokinetic profiling)
Excipients
No proprietary excipient used
1.5 mL of prefilled ozempic injection contains: 1. Disodium phosphate dihydrate 2. 1.42 mg; propylene glycol, 3. 14.0 mg phenol, 4. 5.50 mg water for injections
No residual solvent used
Delivery device(s)
No delivery device
Publications
Wilding, J. P. H., Batterham, R. L., Calanna, S., Davies, M., Van Gaal, L. F., Lingvay, I., McGowan, B. M., Rosenstock, J., Tran, M. T. D., Wadden, T. A., Wharton, S., Yokote, K., Zeuthen, N., Kushner, R. F., & STEP 1 Study Group (2021). Once-Weekly Semaglutide in Adults with Overweight or Obesity. The New England journal of medicine, 384(11), 989–1002. https://doi.org/10.1056/NEJMoa2032183
Background: Obesity is a global health challenge with few pharmacologic options. Whether adults with obesity can achieve weight loss with once-weekly semaglutide at a dose of 2.4 mg as an adjunct to lifestyle intervention has not been confirmed.
Methods: In this double-blind trial, we enrolled 1961 adults with a body-mass index (the weight in kilograms divided by the square of the height in meters) of 30 or greater (≥27 in persons with ≥1 weight-related coexisting condition), who did not have diabetes, and randomly assigned them, in a 2:1 ratio, to 68 weeks of treatment with once-weekly subcutaneous semaglutide (at a dose of 2.4 mg) or placebo, plus lifestyle intervention. The coprimary end points were the percentage change in body weight and weight reduction of at least 5%. The primary estimand (a precise description of the treatment effect reflecting the objective of the clinical trial) assessed effects regardless of treatment discontinuation or rescue interventions.
Results: The mean change in body weight from baseline to week 68 was -14.9% in the semaglutide group as compared with -2.4% with placebo, for an estimated treatment difference of -12.4 percentage points (95% confidence interval [CI], -13.4 to -11.5; P<0.001). More participants in the semaglutide group than in the placebo group achieved weight reductions of 5% or more (1047 participants [86.4%] vs. 182 [31.5%]), 10% or more (838 [69.1%] vs. 69 [12.0%]), and 15% or more (612 [50.5%] vs. 28 [4.9%]) at week 68 (P<0.001 for all three comparisons of odds). The change in body weight from baseline to week 68 was -15.3 kg in the semaglutide group as compared with -2.6 kg in the placebo group (estimated treatment difference, -12.7 kg; 95% CI, -13.7 to -11.7). Participants who received semaglutide had a greater improvement with respect to cardiometabolic risk factors and a greater increase in participant-reported physical functioning from baseline than those who received placebo. Nausea and diarrhea were the most common adverse events with semaglutide; they were typically transient and mild-to-moderate in severity and subsided with time. More participants in the semaglutide group than in the placebo group discontinued treatment owing to gastrointestinal events (59 [4.5%] vs. 5 [0.8%]).
Conclusions: In participants with overweight or obesity, 2.4 mg of semaglutide once weekly plus lifestyle intervention was associated with sustained, clinically relevant reduction in body weight. (Funded by Novo Nordisk; STEP 1 ClinicalTrials.gov number, NCT03548935).
Garvey, W. T., Batterham, R. L., Bhatta, M., Buscemi, S., Christensen, L. N., Frias, J. P., Jódar, E., Kandler, K., Rigas, G., Wadden, T. A., Wharton, S., & STEP 5 Study Group (2022). Two-year effects of semaglutide in adults with overweight or obesity: the STEP 5 trial. Nature medicine, 28(10), 2083–2091. https://doi.org/10.1038/s41591-022-02026-4
The STEP 5 trial assessed the efficacy and safety of once-weekly subcutaneous semaglutide 2.4 mg versus placebo (both plus behavioral intervention) for long-term treatment of adults with obesity, or overweight with at least one weight-related comorbidity, without diabetes. The co-primary endpoints were the percentage change in body weight and achievement of weight loss of ≥5% at week 104. Efficacy was assessed among all randomized participants regardless of treatment discontinuation or rescue intervention. From 5 October 2018 to 1 February 2019, 304 participants were randomly assigned to semaglutide 2.4 mg (n = 152) or placebo (n = 152), 92.8% of whom completed the trial (attended the end-of-trial safety visit). Most participants were female (236 (77.6%)) and white (283 (93.1%)), with a mean (s.d.) age of 47.3 (11.0) years, body mass index of 38.5 (6.9) kg m-2 and weight of 106.0 (22.0) kg. The mean change in body weight from baseline to week 104 was -15.2% in the semaglutide group (n = 152) versus -2.6% with placebo (n = 152), for an estimated treatment difference of -12.6 %-points (95% confidence interval, -15.3 to -9.8; P < 0.0001). More participants in the semaglutide group than in the placebo group achieved weight loss ≥5% from baseline at week 104 (77.1% versus 34.4%; P < 0.0001). Gastrointestinal adverse events, mostly mild-to-moderate, were reported more often with semaglutide than with placebo (82.2% versus 53.9%). In summary, in adults with overweight (with at least one weight-related comorbidity) or obesity, semaglutide treatment led to substantial, sustained weight loss over 104 weeks versus placebo. NCT03693430.
Frías, J. P., Auerbach, P., Bajaj, H. S., Fukushima, Y., Lingvay, I., Macura, S., Søndergaard, A. L., Tankova, T. I., Tentolouris, N., & Buse, J. B. (2021). Efficacy and safety of once-weekly semaglutide 2·0 mg versus 1·0 mg in patients with type 2 diabetes (SUSTAIN FORTE): a double-blind, randomised, phase 3B trial. The lancet. Diabetes & endocrinology, 9(9), 563–574. https://doi.org/10.1016/S2213-8587(21)00174-1
Background: Semaglutide is an effective treatment for type 2 diabetes; however, 20-30% of patients given semaglutide 1·0 mg do not reach glycaemic treatment goals. We aimed to investigate the efficacy and safety of once-weekly semaglutide 2·0 mg versus 1·0 mg in adults with inadequately controlled type 2 diabetes on a stable dose of metformin with or without a sulfonylurea.
Methods: We did a 40-week, randomised, active-controlled, parallel-group, double-blind, phase 3B trial (SUSTAIN FORTE) at 125 outpatient clinics in ten countries. Participants (≥18 years) with inadequately controlled type 2 diabetes (HbA1c 8·0-10·0%) with metformin and with or without sulfonylurea were randomly assigned (1:1) by an interactive web-response system to 2·0 mg or 1·0 mg once-weekly semaglutide. Participants, site personnel, the clinical study group, and investigators were masked to the randomised treatment. Outcomes included change from baseline at week 40 in HbA1c (primary outcome) and bodyweight (secondary confirmatory outcome), evaluated through trial product estimand (no treatment discontinuation or without rescue medication) and treatment policy estimand (regardless of treatment discontinuation or rescue medication) strategies. This study is registered with ClinicalTrials.gov, NCT03989232; EudraCT, 2018-004529-96; and WHO, U1111-1224-5162.
Findings: Between June 19 and Nov 28, 2019, of 1515 adults assessed for eligibility, 961 participants (mean age 58·0 years [SD 10·0]; 398 [41%] women) were included. Participants were randomly assigned to once-weekly semaglutide 2·0 mg (n=480 [50%]) or 1·0 mg (n=481 [50%]); 462 (96%) patients in the semaglutide 2·0 mg group and 471 (98%) in the semaglutide 1·0 mg group completed the trial. Mean baseline HbA1c was 8·9% (SD 0·6; 73·3 mmol/mol [SD 6·9]) and BMI was 34·6 kg/m2 (SD 7·0). Mean change in HbA1c from baseline at week 40 was -2·2 percentage points with semaglutide 2·0 mg and -1·9 percentage points with semaglutide 1·0 mg (estimated treatment difference [ETD] -0·23 percentage points [95% CI -0·36 to -0·11]; p=0·0003; trial product estimand) and -2·1 percentage points with semaglutide 2·0 mg and -1·9 percentage points with semaglutide 1·0 mg (ETD -0·18 percentage points [-0·31 to -0·04]; p=0·0098; treatment policy estimand). Mean change in bodyweight from baseline at week 40 was -6·9 kg with semaglutide 2·0 mg and -6·0 kg with semaglutide 1·0 mg (ETD -0·93 kg [95% CI -1·68 to -0·18]; p=0·015; trial product estimand) and -6·4 kg with semaglutide 2·0 mg and -5·6 kg with semaglutide 1·0 mg (ETD -0·77 kg [-1·55 to 0·01]; p=0·054; treatment policy estimand). Gastrointestinal disorders were the most commonly reported adverse events (163 [34%] in the 2·0 mg group and 148 [31%] in the 1·0 mg group). Serious adverse events were similar between treatment groups, reported for 21 (4%) participants given semaglutide 2·0 mg and 25 (5%) participants given semaglutide 1·0 mg. Three deaths were reported during the trial (one in the semaglutide 1·0 mg group and two in the semaglutide 2·0 mg group).
Interpretation: Semaglutide 2·0 mg was superior to 1·0 mg in reducing HbA1c, with additional bodyweight loss and a similar safety profile. This higher dose provides a treatment intensification option for patients with type 2 diabetes treated with semaglutide in need of additional glycaemic control.
Additional documents
No documents were uploaded
Useful links
There are no additional links
Collaborate for development
Consider on a case by case basis, collaborating on developing long acting products with potential significant public health impact, especially for low- and middle-income countries (LMICs), utilising the referred to long-acting technology
Share technical information for match-making assessment
Provide necessary technical information to a potential partner, under confidentiality agreement, to enable preliminary assessment of whether specific medicines of public health importance in LMICs might be compatible with the referred to long-acting technology to achieve a public health benefit
Work with MPP to expand access in LMICs
In the event that a product using the referred to long-acting technology is successfully developed, the technology IP holder(s) will work with the Medicines Patent Pool towards putting in place the most appropriate strategy for timely and affordable access in low and middle-income countries, including through licensing